ADvancing States and the Center for Health Care Strategies (CHCS) partnered to develop a series of short briefs to inform adoption of state strategies that better align Medicare and Medicaid for dually eligible beneficiaries. The Value of Pursuing Medicare-Medicaid Integration for Medicaid Agencies, which HHAeXchange has summarized here, is the first in the series of three briefs.
State Medicaid officials from Arizona, Connecticut, Maine, Massachusetts, Minnesota, Ohio, Pennsylvania, Virginia, Tennessee, and Washington shared their perspective to inform the brief.
Overview
People who are dually eligible for Medicare and Medicaid must navigate two uncoordinated systems of care with different incentives, benefits, provider networks, and enrollment processes. Approximately 60 percent of dually eligible beneficiaries have multiple chronic conditions, more than 40 percent have at least one mental health diagnosis, and nearly half of individuals eligible for both programs use long-term services and supports (LTSS).
As of October 2019, more than one-third of states operate Medicare-Medicaid integrated care models that have substantial enrollment in demonstrations under the Financial Alignment Initiative (FAI) or Dual Eligible Special Needs Plans (D-SNPs) that are aligned with Medicaid managed care plans, an increase from three states in 2009.
Dual Eligible Characteristics
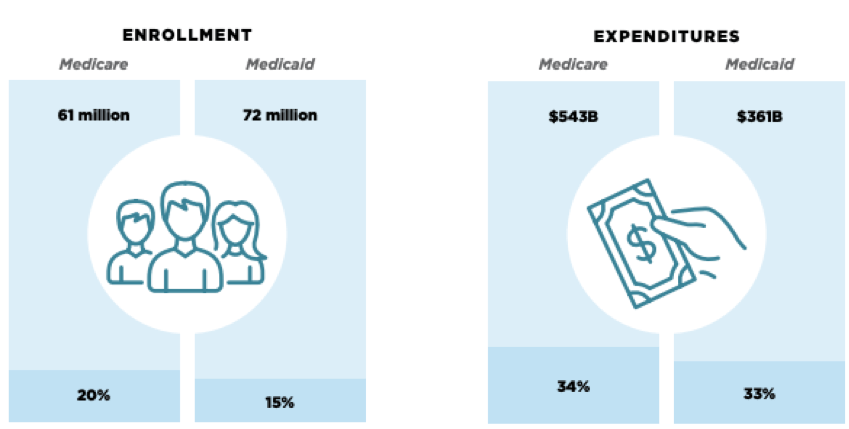
Source: ADvancing States
There are new opportunities for states to explore integrated care models for dually eligible beneficiaries, a diverse but high-need, high-cost population. There are some promising findings for states that are considering new integrated care models, which include:
-
Improved beneficiary experience, health outcomes, and quality of life due to closer coordination across different providers, systems, payers, social supports;
-
Increased program efficiencies due to aligned financial incentives to provide person-centered care in the right setting at the right time; and
-
Improved Medicaid program administration and management due to better access to Medicare data and increased capacity to better manage this high-need, high-cost population.
Integrated care models may differ in their care management approach and the level of administrative and financial alignment achieved, but have the same overarching goals of integrating primary, acute, and behavioral health services with LTSS.
More states are exploring the possibility of establishing an integrated care option, but most have yet to act. Establishing an integrated care program requires considerable state resources and investment in staffing and systems, as well as stakeholder engagement. Also, historically, savings from reduced acute care service use achieved through better care coordination have accrued to Medicare, not state Medicaid programs. To make the case for integration, states need a clear picture of the value that these programs can bring to their Medicaid agencies and the beneficiaries they serve.
Findings on the Value of Integration
Beneficiary Experience. One state affirmed that the public good of creating an integrated benefit for a complex population far outweighed the relative costs of setting up the program. Another commented that from a consumer standpoint, it makes no sense for people to be in separate, unconnected programs that create barriers to coordinated, high-quality care.
Self-Reported Beneficiary Satisfaction. High satisfaction rates may be due in part to less beneficiary confusion, fewer issues with coordinating authorizations across different entities for important services, and avoided delays in care from aligning services under one entity or program.
Care Coordination. In integrated programs, one entity coordinates the full range of medical and behavioral health as well as LTSS needs. Investments in care coordination at the health plan and provider levels – particularly as individuals move from institutional settings to home – can both reduce unnecessary hospitalization and other adverse health events, and keep people at home longer.
Quality of Care. Many integrated programs demonstrate improved health outcomes, typically through better management of Medicare-covered primary or acute care services. Medicaid agencies have a great interest in ensuring that dually eligible beneficiaries are as healthy as possible. In particular, better management of chronic conditions can prevent or deter utilization of Medicaid-covered LTSS.
At HHAeXchange, we view the caregiver in the home as a critical part of the care team for dual eligible members, and we are focused on delivering technology solutions that integrate caregiver observations with the broader care team. With over 536,000 caregivers utilizing our EVV tools, collecting information at the point of care and delivering that back to the agency care team for monitoring is a natural extension of our technology.
Medicaid Program Efficiency
Long-Term Services and Supports Utilization. A disproportionate amount of LTSS spending is driven by institutional care costs. Encouraging appropriate LTSS utilization by dually eligible beneficiaries – focusing on skilled nursing facility (SNF) admissions and long stays in nursing facilities (NF) – is a high priority for states eager to reduce LTSS cost growth.
One study found that dually eligible individuals are 12 percent more likely to become long-stay NF residents and use more SNF care compared to Medicare-only patients, underscoring the importance of managing appropriate utilization of both SNF and NF services.
Since spending on Medicaid LTSS is projected to grow due to an anticipated 50 percent increase in individuals age 65 and older by 2030, continuing to shift the balance of LTSS to community-based care is critical for states.
Program Administration. Many of the interviewed states are analyzing utilization patterns and health care needs of individuals at risk of becoming dually eligible to identify opportunities for early interventions that deter higher service needs down the road. CMS has developed a new Transformed Medicaid Statistical Information System that will provide needed information about Medicaid spending and utilization in these programs.
The Need for Integrated Care:
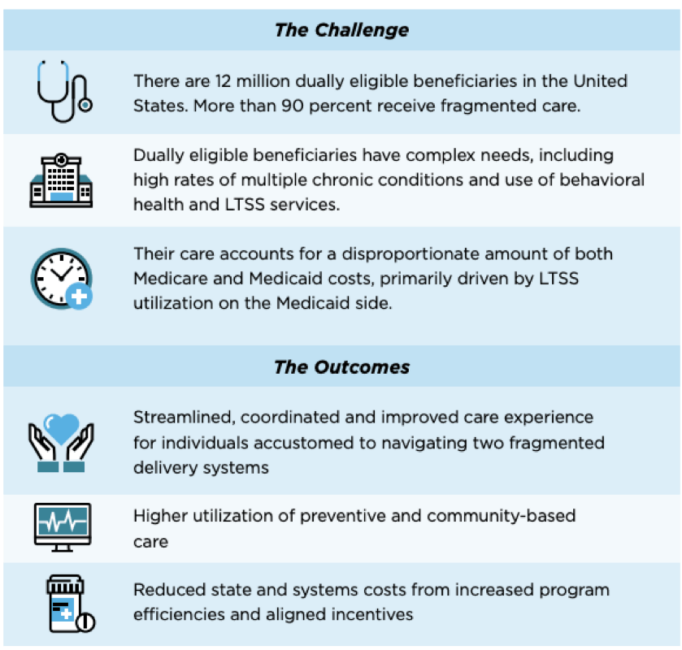
Source: ADvancing States
Conclusion
There is a growing body of data supporting the value of integrated care programs for Medicaid agencies. This is focused on better care experience, shifting of Medicaid LTSS utilization to lower-cost, community-based services, and improvements in program administration.
As many state interviewees noted, the investments needed in staffing, system resources, and stakeholder engagement for these programs are significant factors that dictate program success. One interviewee said, “These programs are worth it, and you get back what you put in.”
This post was updated on Wed Oct 15 2025.


