Updates: New York has received a Good Faith Effort (GFE) exemption to delay EVV implementation to January 1, 2021.
New York has elected to proceed with the Choice Model for implementing EVV.
The New York State Department of Health (NYSDOH) recently released its EVV Stakeholder Report. The report, which was part of NYSDOH’s efforts to successfully plan and implement EVV in time for the Cures Act mandate, summarized the information gathered from in-person Listening Sessions with providers and surveys conducted to assess the current landscape around EVV in NY.
Some of the main themes that emerged during the regional Listening Sessions included: issues and concerns regarding privacy and security, accessibility and availability, cost and funding, timelines, decision-making, training, and potential impacts of the EVV program.
Survey Findings
The EVV Survey was delivered to New York providers who billed Medicaid for more than $100,000 of Personal Care Services and/or Home Health Care Services in 2018. NYDSOH achieved a 20% response rate consisting of 146 total responses. Here is a snapshot of some of the survey’s findings:
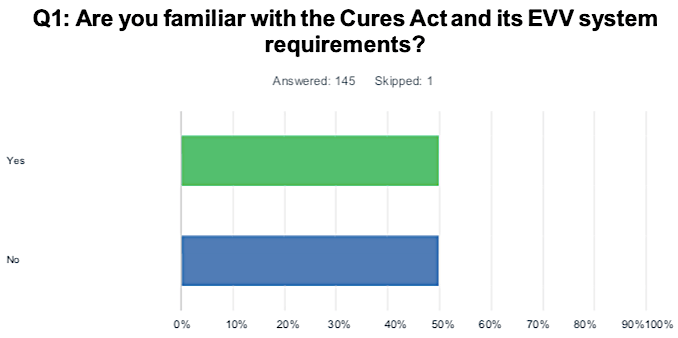
Source: New York State Department of Health
While one-half of the survey respondents were aware of the EVV mandate under the Cures Act, the other half were not. Though EVV has been around for more than twenty years, with the passing of the 21st Century CURES Act, EVV is now a requirement for Medicaid homecare providers. The CURES Act requires homecare visits to be electronically verified for the type, date, and location of the service being performed; the individual receiving the service; the caregiver or aide performing the service, and the time the service begins and ends.
For more information about EVV and the Cures Act, check out our blog post: How to Prepare for the 21st Century Cures Act.
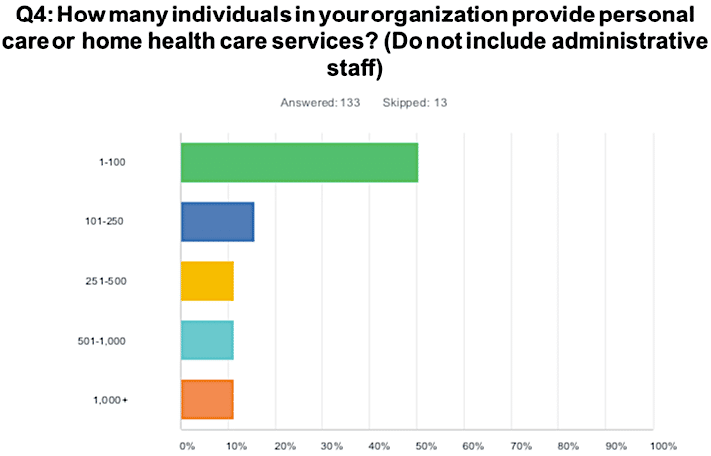
Source: New York State Department of Health
About 50% of the stakeholders surveyed are part of organizations with 1-100 individuals providing personal care or home health services. Slightly over 10% of providers surveyed have more than 1,000 aides in their organization.
Larger providers may be better equipped to adopt and implement EVV, whereas smaller providers could be more challenged as they may not have the additional resources needed to carry out the change. With that being said, smaller providers have fewer employers and caregivers to train, which could potentially allow for an easier transition.
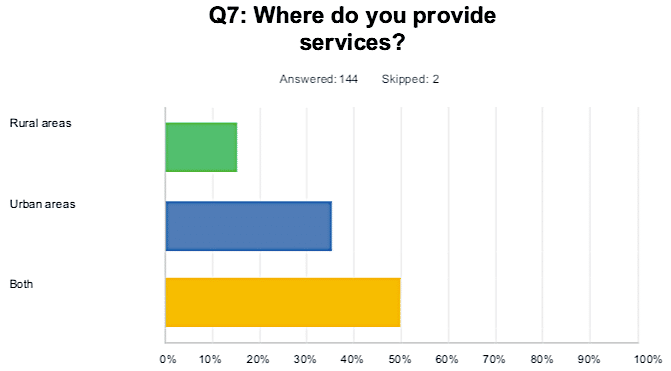
Source: New York State Department of Health
Of the 144 survey respondents, 22 provide services in rural areas, 51 provide services in urban areas, and 71 provide services in both rural and urban areas.
During the Listening Sessions, some providers pointed out that geographic areas with limited or no internet or cellular connectivity (“dead-zones”) could face a challenge with EVV. Without a cellular or internet connection, they wondered how an EVV system will collect data and send it to the system’s server in a timely manner.
However, there are several leading EVV technologies in place today that account for low or no-service areas. For example, the HHAeXchange mobile app has an offline mode which caregivers can use to clock-in and clock-out in areas without any service, as well as a Bluetooth Beacon device that can be placed in the patient’s home and paired with the Mobile App or telephony for clocking in and out.
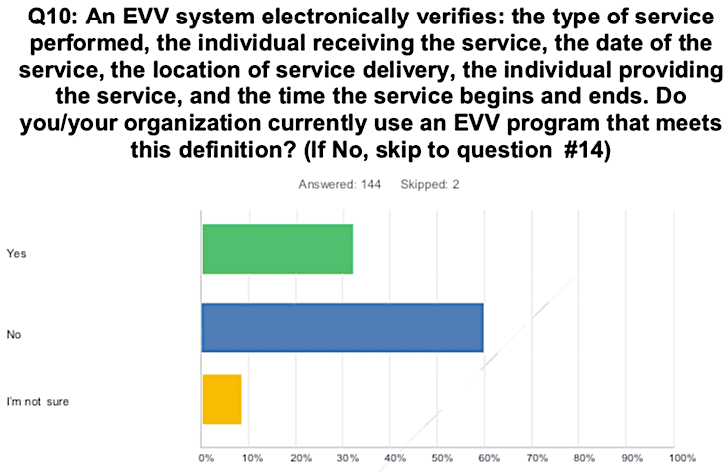
Source: New York State Department of Health
Forty-six survey respondents indicated they now have EVV in place. Those respondents reported employing a wide range of existing EVV technologies, infrastructure, and processes. Thirty-two percent of those with an EVV in place reported their current EVV solution is compliant with the Cures Act. The EVV technologies they’re currently using include: non-smartphone cell phones, applications accessed through smartphones, in-home key fobs, and landlines.
Approximately one-half of those respondents with an EVV solution in place reported using GPS in EVV data collection, and over two-thirds utilize EVV systems that incorporate functionality in addition to that required by the Cures Act including: scheduling, reporting, claims submission, billing, and authorization.
Source: New York State Department of Health
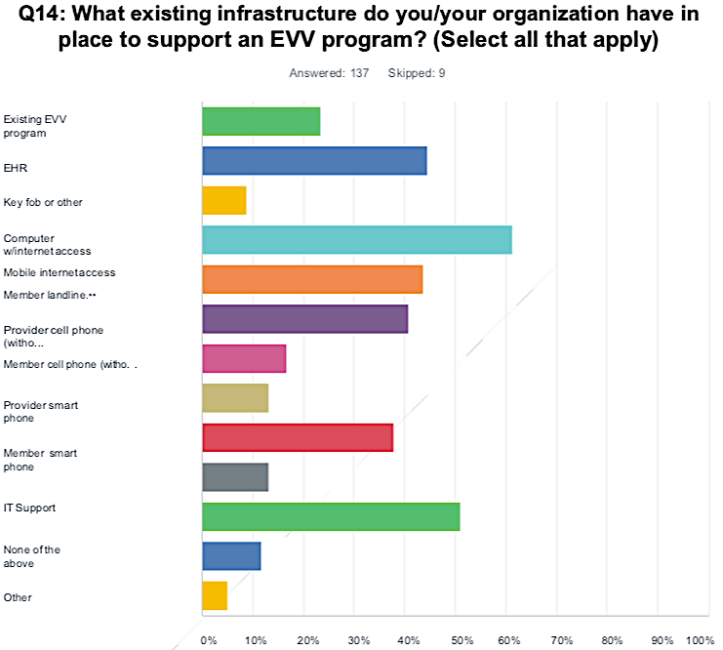
Survey respondents reported having a variety of existing infrastructure in place to support an EVV program, including but not limited to: an existing EVV solution, a computer with internet access, member landline, member smartphone, IT support, key fob or other device.
While some providers raised concerns about various aspects of EVV technologies and systems during the Listening Sessions, others said that once fully implemented, EVV systems would be an asset in helping them meet quality measures and standards. Some providers also indicated that the use of GPS and geofencing can be beneficial because they ensure consumers receive the services they need and allow agencies to be alerted if an aide does not show up for their shift. This kind of information, they noted, can assist agencies with making necessary adjustments in scheduling and staffing in order to ensure any patient that needs an aide that day has one.
Additionally, many providers presented examples of how their EVV systems have been configured to address some of the concerns raised. For example, providers explained that EVV systems that use GPS to collect location data do not continuously track throughout the duration of the service; rather the GPS is only functional when the caregiver is clocking the start and end times of the shift.
Next Steps
The Cures Act mandate includes a provision that allows states to delay implementation of EVV for up to one year if they can demonstrate they have made a Good Faith Effort (GFE) to comply and have encountered unavoidable delays. On October 30, 2019, the DOH submitted a request for a one–year GFE extension from the Centers for Medicare and Medicaid Services (CMS), which can be found here. The EVV website will be updated in the future to reflect CMS´s determination.
The EVV Stakeholder Report, and the information gathered through the Listening Sessions and provider surveys, mark NYSDOH’s first milestone in planning and implementing EVV in compliance with the federal mandate. The other three milestones are as follows:
-
2nd Milestone: Formulating EVV implementation options, taking into consideration the input received from milestone one, developing a strategy and executing a strategy.
-
3rd Milestone: Implementation of the selected option, including but not limited to technology, cost, training, and working with an EVV vendor or vendors, if necessary.
-
4th Milestone: Evaluation and monitoring of the implemented operation
To receive future EVV updates from NYSDOH and to offer your input on the State’s implementation of EVV:
-
Visit NY’s EVV webpage
-
Sign up for NY’s EVV Listserv by emailing [email protected] with the following: SUBSCRIBE EVV-L YourFirstName YourLastName
-
Email the NYSDOH EVV help desk at [email protected]
To view the full Stakeholder Convening Report, click here.
HHAeXchange is the industry leader in providing EVV solutions across the country with over 104.9 million visits confirmed annually through our platform. Contact us today to learn more about EVV in New York and ensure you’re prepared to meet the Cures Act deadline.
This post was updated on Wed Oct 15 2025.

