Where does your clinical documentation live? If the answer is in binders, spreadsheets, or a standalone software, you’re not alone—but it could be impacting your care quality. It’s great that the care is getting documented, but without a centralized location, those records end up in a documentation black hole, making them hard to act on, and nearly impossible to audit.
Our newly enhanced product, HHAeXchange Clinical, solves this. Available in HHAeXchange Enterprise, it lets caregivers document medication administration, vital signs, wound care, and clinical forms directly in the HHAeXchange+ mobile app—and makes all of it instantly visible to administrators in the platform. The result is a shift from collecting notes to maintaining reliable clinical records your agency can actually use.
From Scattered Notes to a Clinical Record You Can Trust
Most homecare agencies aren’t struggling because caregivers aren’t documenting—they’re struggling because that documentation doesn’t go anywhere useful. A paper medication administration record filed in a binder, vital signs scribbled on a visit note, wound photos texted to a supervisor: the information exists, but it’s not connected, not reviewable, and not audit-ready.
HHAeXchange Clinical changes the structure, not just the format. When caregivers document through the HHAeXchange+ app, every entry is automatically tied to the visit where it occurred, time-stamped, and immediately available to your administrative team. There’s no manual reconciliation, no chasing down records before an audit, and no ambiguity between what a caregiver observed and what your team can see.
For agency owners, this matters beyond compliance. When your clinical picture is complete and current, your team can spot changes in condition earlier, respond faster, and reduce the kind of avoidable escalations that drive up costs, strain staff, and worsen client health outcomes. Good documentation infrastructure is a competitive advantage—and now it’s built into the platform you’re already using.
WhatHHAeXchange Clinical Offers:
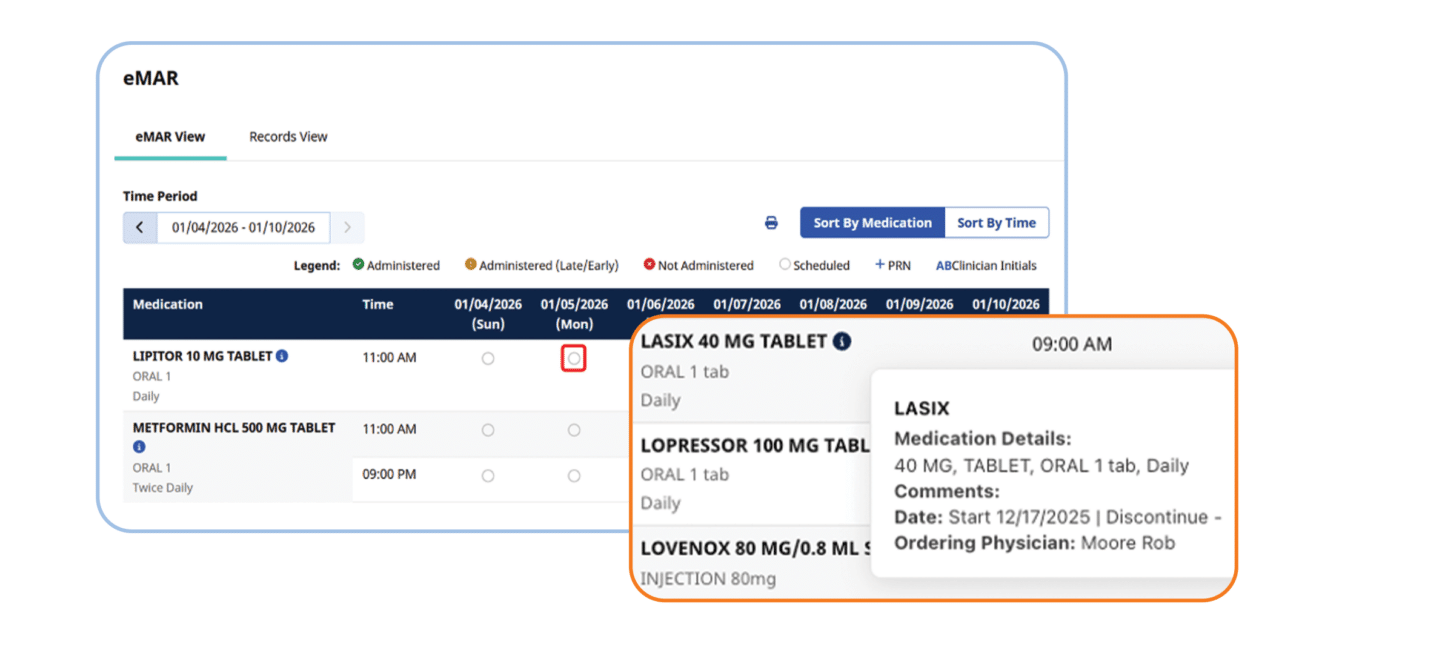
eMAR (Electronic Medication Administration Records): Replace paper medication files with a single digital record tied to each visit. Caregivers can log scheduled, administered, or missed medications during the visit, and every entry—including corrections—is captured in a full audit trail.
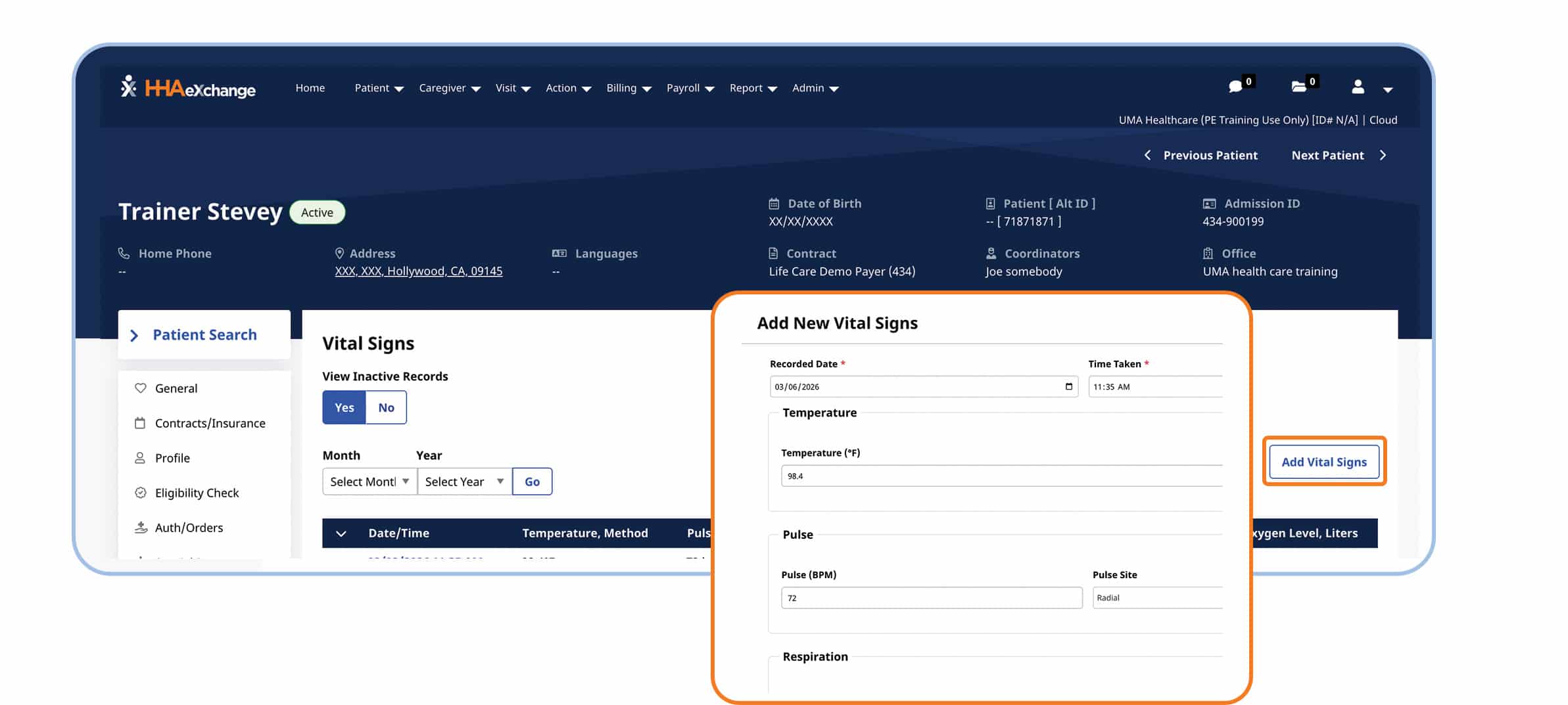
Vital Signs: Caregivers record vital signs during visits, and your team can track history and trends directly in the patient record. Out-of-range values are flagged automatically, so your clinical staff can follow up before a small change becomes a larger problem.
Wound Tracking: Document wound measurements, status, and photos at every visit. Healing progress is tracked across visits and caregivers, giving your team a clear, continuous record of reassessments and changes over time.
Forms: Easily build your own from scratch or choose from our template library to match your agency’s needs. Designed to be easy for both caregivers and office staff, forms auto-populate from patient and visit records and guide caregivers through required fields so critical information isn’t missed. This reduces back-and-forth between caregivers and agencies to correct incomplete documentation, while built-in version control ensures consistency over time. The result is structured, audit-ready documentation that paper and PDFs simply can’t provide.
Ready to See It in Action?
HHAeXchange Clinical is available now for Enterprise customers. If you’re ready to bring your clinical documentation out of the black hole and into a system that actually works for your agency, request a demo today.
This post was updated on Tue May 05 2026.


